


Breast Reconstruction, including Timing, and Reconstruction Rates
Breast reconstruction is a procedure carried out to restore breast shape and replace breast tissue lost during a mastectomy. The goal is to match the opposite breast as closely as possible, or, in some cases, to create a pair of breasts that are symmetrical and natural looking and, if possible, resemble the patient’s original breasts.
Breast reconstruction surgery aims to restore the appearance of a natural breast after a mastectomy—and can help a woman look and feel like her normal self again. Many women find that breast reconstruction significantly improves their self-image, self-confidence and quality of life. On the practical side, breast reconstruction eliminates the need for external artificial prostheses, which can sometimes be uncomfortable and awkward to wear.

It is never an easy task to make important surgical decisions in the face of a breast cancer diagnosis, especially when there is an overwhelming amount of information presented to you by doctors, family, and friends. A well-informed patient who actively participates in decision making is an essential ingredient of successful outcome in breast reconstruction. The surgeons must be prepared to answer all the patient’s questions in a clear and concise manner. All women considering breast reconstruction need to understand the rationale for reconstruction and have realistic expectations for what can be accomplished. They need to consider the optimal timing and the advantages and disadvantages of each technical option.
Once a decision has been made to proceed with mastectomy, or even if mastectomy is simply an option being explored, the discussion of breast cancer reconstruction should naturally follow. A 2007 study showed that the option of breast reconstruction is intimately tied to patients’ choice of surgery, underscoring the importance of informing patients about the option of breast reconstruction before initial surgical choice. Cancer,2007.

While it is normal to feel a sense of urgency to want the cancer removed immediately, it is important to make educated and informed decisions that are not rushed. Taking a few weeks from the biopsy to the surgery is very unlikely to have any impact (see section Delay between Diagnosis and Surgery).
For most patients, reconstruction will require from one to three or more procedures to achieve the desired result. The first procedure is usually the most lengthy and complex, while the other procedures tend to be more minor. Although reconstructive surgery is secondary to other
treatments that are directly related to survival, it is, for many women, an essential part of recovery and return to normal living. It should therefore not be considered frivolous or a matter of vanity. Secondly, any women considering breast reconstruction must understand that choosing it is more than simply electing to have a surgical procedure. As outlined above, it typically involves more than one surgical procedure, and frequent visits may be necessary over a period of many months. Complications may occur that require treatment or unplanned procedures. Final results often require many months to realize, depending on the technique of reconstruction. One of the most important factors for successful decision making is to determine the patient’s degree of willingness to engage in this process. The patient must understand this and be agreeable and committed to the process.

Although the goal of breast reconstruction is to match a woman’s previous breast(s) as closely
as possible, patients must bear in mind that the procedure will not precisely restore the original
appearance and shape. The reconstructed breast will not have the same sensation, and lactation is not possible in the reconstructed breast.
It is also important that women are reassured and made aware that reconstructive breast surgery does not interfere with the future detection of any breast cancer recurrence and that breast reconstruction does not increase the risk of breast cancer recurrence.
Breast reconstruction is an option and never an essential part of treatment, however the option of breast reconstruction should be explored with every woman having a mastectomy. Although breast reconstruction should be discussed with all women who are having a mastectomy, not all women will be suitable candidates for an immediate reconstruction.

Breast reconstruction is a highly individualized procedure. You should do it for yourself, not to fulfill someone else’s desires or to try to fit any sort of ideal image. The important thing is that it is your choice. Talking to other women who have undergone treatment can often help you decide whether or not breast reconstruction is the right option for you.
TIMING OF RECONSTRUCTION
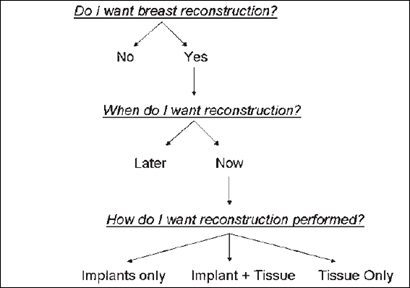
One of the first choices you will need to make is whether you want a reconstruction at all. The basic “decision tree” for breast reconstruction candidates consists of three essential questions (see table below) After deciding to have breast reconstruction, the next decision is to choose the timing. Each woman needs to understand the rationale for choosing to have reconstruction performed at the same time as the mastectomy (immediate reconstruction) or later, after recovery from surgery and completion of any associated treatments (delayed reconstruction)
The best candidates for immediate reconstruction are women in general good health with early-stage disease.
No reconstruction
Choosing not to have breast reconstruction is, of course, a very satisfactory option for some women. Many women feel radically changed by their cancer experience, and some feel that a flat chest is an apt acknowledgement and expression of their post-cancer persona. Others are very satisfied choosing to wear a prosthetic breast in their bra rather than have to undergo more surgery, although some women find it restricts their choice of clothing. Some may simply prefer to avoid further surgery. Others wish to minimize the possibility of inconvenience associated
with treating complications. In these women, it is best to defer reconstruction. This is certainly the best option for any woman who simply cannot make a decision regarding reconstruction or who maintains unrealistic expectations about the outcome.

If you are going to have a breast reconstruction, you should aim to have a good one. A poor reconstruction may, in many circumstances, be worse than none at all. Although there can obviously be no guarantees, in general, the quality/result of breast reconstruction surgery is directly related to the skill, experience and expertise of the surgeons involved. A team approach, with close collaboration between the breast surgeon and plastic surgeon is essential, with consideration given to both oncological and reconstructive aspects, especially in the setting of immediate reconstruction. Teams of breast and plastic surgeons who operate jointly together on a regular basis become very familiar with their colleague’s treatment approaches. The plastic surgeon will then be aware of what has been previously discussed between the breast surgeon and the patient and can reinforce important issues relating to the cancer treatment. This familiarity and experience results in the patient receiving a unified message, minimising the chance of the patient receiving conflicting, mixed messages about the appropriate treatment options.
The surgeons must not only provide fundamental technical information about the surgery, (eg options, possible complications, additional procedures etc) but also assist the patient in clarifying her personal goals and priorities. Patients with significant major comorbidities who are not good surgical candidate typically may not undergo reconstruction. Another relative contraindication to breast reconstruction is unrealistic patient expectations. Thus, an important component of the consultation and evaluation process is addressing patient desires and expectations. A well informed patient is much more likely to have realistic expectations and be satisfied with the final result.

Currently, the majority of breast reconstructions are performed as immediate reconstructions at the time of mastectomy. This usually produces the optimal aesthetic result since it allows for preservation of the breast skin envelope, inframammary fold and sometimes for nipple preservation (see Nipple-Sparing Mastectomy).
Immediate reconstruction
The benefits of immediate reconstruction are:
- The cosmetic results are usually better
- More of the skin of your breast can be preserved (and also the nipple on occasions)
- The scarring on the breast itself is usually less
- You will not have to spend any time without a breast mound

Not all women will be suitable/ideal candidates for an immediate reconstruction. Delayed reconstruction is indeed a preferable option for some patients. Women with health problems such as obesity, high blood pressure and diabetes may be advised to wait. There is a very significantly increased risk of complications after reconstructive surgery in smokers, and smoking should be considered a relative contraindication to breast reconstruction. On occasions immediate reconstruction may not be recommended if it is felt that the level of increased risk of complications, such as in obese smokers for example, is such that chemotherapy may potentially be delayed. Unexpected complications can of course always occur, even in women not felt to be at high risk, however reassuringly the literature, including a local Melbourne study, The Breast,2013, suggests that reconstructive surgery at the time of mastectomy does not significantly delay initiation of adjuvant chemotherapy.
Those who are overwhelmed by the diagnosis of breast cancer and the discussion of both surgical and medical approaches to treatment may not be able to make a sound decision regarding their preferences for breast reconstruction at the time of mastectomy. For such patients, a step-by-step approach that addresses tumour management first and the reconstructive procedures later may be more appropriate.

There’s one really important piece of advice if you are thinking about reconstruction. If you really can’t make up your mind about whether to go ahead, don’t feel cornered into making a snap decision. Ask for more information. There are lots of helpful sources of information –one of the most valuable is to speak to other patients who have had to make the same decisions as you. They will tell you about their own experiences and reactions and their recovery.
If you still feel unable to make up your mind, then it’s probably wisest not to go ahead with an immediate reconstruction. If you feel pressurised to go ahead and things go wrong, you’ll wish you had never had it done. You can always have a new breast at a later date once you have had a chance to get over your treatment and return to normal. The timing of breast reconstruction is a very individual choice and there are many different factors in deciding which choice is best for you and your own particular circumstances. Finally, if you need another week or two to make up your mind, don’t be afraid to ask for more time. It’s not going to make the slightest difference to your chances of recovery, and may just be the time you need to be sure you’ve made the best decision for you.
Delayed reconstruction
The benefits of delayed reconstruction are:
- Your cancer treatment can proceed without delay
- There is more time to consider whether reconstruction is right for you
- There is less for you to deal with, all at once

The need for postoperative radiation therapy is a relative contraindication to immediate breast reconstruction using certain techniques. Radiotherapy has an unpredictable effect on the outcome of both implant-based and autogenous tissue–based reconstruction. Radiotherapy to the reconstructed breast results in tissue damage, disfigurement, and can precipitate complications in both flap-based and implant-based reconstructions. If the administration of adjuvant radiotherapy is anticipated, many plastic surgeons have concerns regarding reconstruction with either implants or autogenous tissue because of the potential for significant capsular contracture in implant reconstructions and severe fibrosis or atrophy of the autogenous-tissue flap. It is important that the patient understand how radiation therapy affects the timing of reconstruction. When radiation is not anticipated, immediate reconstruction is very often the preferred option. For most women it yields more natural-appearing results compared with delayed reconstruction.
When radiation therapy is required, it may be preferable to have delayed reconstruction after completing radiation treatments. In general, reconstruction is often delayed for 6-12 months after radiation therapy is complete to allow tissue healing and to appreciate fully the extent of postradiation damage to the tissue. It is important for mastectomy patients to know that they are still candidates for breast reconstruction as a delayed procedure, even if their mastectomy was performed in the distant past.
Post mastectomy radiation is generally reserved for women at higher risk of local recurrence. Currently, post mastectomy radiotherapy is recommended to women who have 4 or more involved nodes, a tumour more than 5cm or skin or chest wall involvement. Women with 1-3 positive axillary nodes are considered for post mastectomy radiotherapy on an individual basis.
In patients requiring radiotherapy who still express a strong preference for immediate reconstruction, it may be advisable to reconstruct the breast with a larger volume to offset postradiation tissue atrophy and fibrosis. In many patients, in fact, the need for radiotherapy is uncertain until the operative pathology is available. Under these circumstances, the patient might consider a ‘‘delayed-immediate’’ reconstruction method, in which a tissue expander is temporarily placed beneath the mastectomy flaps and filled to the appropriate volume needed to preserve the skin envelope during radiation therapy, and the reconstruction delayed until after radiation is complete.

Delayed-immediate reconstruction involves placement of a tissue expander at the time of skin-sparing or nipple- sparing mastectomy in order to preserve the breast skin envelope, using the tissue expander as a ‘‘pocket preserver’’. If radiation therapy is then required, the patient may undergo definitive flap reconstruction, if that is the desired reconstructive method, in a delayed fashion after the radiation therapy is completed. This allows for skin conservation, thereby improving the aesthetic outcome.
There is no doubt that undergoing an immediate reconstruction is in most cases likely to lead to a short delay in the surgery being performed as different surgeons’ schedules have to be coordinated at the same time as a free operating theatre is available, often for a fairly prolonged operation. A 2011 American study found that patients who underwent reconstructive surgery had a median delay from imaging to surgery of 29 days (range, 4–124 days) versus 19 days (range, 1–132) in those who had not undergone reconstructive surgery. Annals of Surgery, 2011.

Findings are similar in the United Kingdom. For women undergoing mastectomy, the average
time from “decision to treat”, to surgery was 20 days, with 87 per cent treated within 31 days. For women having mastectomy with immediate reconstruction, the mean time was 29 days, and only 65 per cent of immediate reconstruction patients were treated within 31 days. Second Report of the National Mastectomy and Breast Reconstruction Audit,2009.
Delays of this magnitude have not been shown to have any impact on cancer outcomes. It is extremely important that patients understand and accept that while all attempts are made to streamline the process as efficiently as possible, pursuing an immediate reconstruction is inevitably very likely to lead to a short delay compared to no reconstruction. If patients are not willing to accept the inevitable short delays associated with the additional information gathering, decision making and scheduling associated with an immediate reconstruction, they are perhaps better served considering the option of a delayed breast reconstruction.

Women undergoing their breast cancer treatment in the public hospital sector should also perhaps consider factoring into their breast reconstruction decision making, the potential waiting times for delayed reconstruction in the public sector. Whilst delayed breast reconstruction following a mastectomy for breast cancer is considered a reconstructive medical procedure ie it is not cosmetic surgery, it is however regarded as elective surgery, usually categorised for waiting list purposes as clinically non urgent, and considerable waiting times, of up to 2 years, for delayed breast reconstruction have been reported in the public sector. ANZJS,2003. In contrast, women who choose to have a reconstruction at the same time as their breast cancer surgery are usually classified as urgent, as there is clinical urgency in performing the breast cancer component of their surgery.
The Breast Care Network Australia (BCNA), Breast Reconstruction Project Report (November 2011) found that ninety-four per cent of the women who completed their survey and who had breast reconstruction through a public hospital, had their surgery within two years of being placed on a waiting list. One acknowledged limitation of the BCNA survey was that only 20 per cent of respondents had their surgery through the public hospital system, so the findings may not have been truly representative of what is happening in the wider community.

RECONSTRUCTION RATES
Breast reconstruction rates differ quite markedly between countries. Internationally, breast-reconstruction rates have been low, with Australia, Denmark, and England reporting national rates of breast reconstruction of 9% (1982–2000), 14% (1999–2006), and 16.5% (2006–2009), respectively. Current evidence suggests that the use immediate breast reconstruction at the time of the mastectomy has steadily increased over time, but currently still remains fairly low.
Reconstruction rates within individual countries also vary significantly by region as well as by patient age, insurance status, and income. In addition, significant disparities exist in the receipt of immediate breast reconstruction by patient race/ethnicity and sociodemographic factors. Limited knowledge, financial barriers, and inadequate referrals to reconstructive surgeons contribute to the low use of immediate breast reconstruction in minority patients.
In the USA, the first large study to look at breast-reconstruction rates using the National Cancer Database reported the reconstruction rate as increasing from 3.4% between 1985-1990 to 8.3% in 1994-1995. J AM Coll Surg, 2001. SEER data from 1998-2002 showed a reconstruction rate of 16.2%, with younger age, white race, metropolitan locale, and lower stage disease, all independently associated with higher likelihood of reconstruction. The Breast,2011.
An analysis of data from the Nationwide Inpatient Sample from 1999 to 2003 showed the average reconstruction rate to be 23.6%. Independent predictors of immediate breast reconstruction after mastectomy included private insurance, hospital in an urban location, teaching hospital, white race, hospital region in the south, age between the 3rd and 6th decades, and absence of comorbidities. Am J Surg, 2009.

In the UK, between 1997 and 2006, the proportion of mastectomy patients undergoing immediate reconstruction rose from 7 per cent to 11 per cent according to data from the First National Mastectomy and Breast Reconstruction Audit, 2007. Data from the 4TH National Mastectomy and Breast Reconstruction Audit,2011 showed that between 2008-2009, 21% of women underwent immediate reconstruction and 11% had delayed reconstruction.
Here in Australia, an audited review published in 1999 indicated that only 6% of Australian women who had mastectomies for breast cancer were receiving breast reconstructions at that time. National Breast Cancer Centre statistics published in 2003 showed that 8% of Australian women who had mastectomies had breast reconstructions and the RACS National Breast Cancer Audit (NBCA) figures for 2007 show that 9.4% of women who underwent a mastectomy during that year had a breast reconstruction.

The proportion of mastectomy cases recorded as receiving immediate reconstruction was 13% for private patients and 6% for public patients. National Breast and Ovarian Cancer Centre and Royal Australasian College of Surgeons National Breast Cancer Audit Public Health Monitoring Series 2008 Data Published August 2010.
The audit statistics showed the percentages of women in each age group who received a breast reconstruction:
- 20% of women aged under 40 who had a mastectomy received breast reconstruction
- 19% of women aged 40-49 who had a mastectomy received breast reconstruction
- 11% of women aged 50-59 who had a mastectomy received breast reconstruction
- 4% of women aged 60-69 who had a mastectomy received breast reconstruction
- 2% of women aged 70-79 who had a mastectomy received breast reconstruction
- No women aged 80 or over who had a mastectomy had a breast reconstruction
The statistics also show that women were more likely to have a reconstruction if they lived in a major city than in an inner regional or more remote location:
- 13% of city women who had a mastectomy received breast reconstruction
- 5% of inner regional women who had a mastectomy received breast reconstruction
- 2% of more remote women who had a mastectomy received breast reconstruction
National Breast and Ovarian Cancer Centre and Royal Australasian College of Surgeons National Breast Cancer Audit Public Health Monitoring Series 2007 Data Published August 2009.

Factors associated with the use of breast reconstruction
What factors influence the utilization of breast reconstruction? The most common factors cited in the literature relate to patient age, race, socioeconomic background, tumour stage, and physician practice. Both surgeon, practice and patient variables may dramatically influence breast reconstruction rates.
Patient Factors
Several studies have demonstrated that younger patient age is the most significant variable associated with an increased likelihood of postmastectomy reconstruction. One possible explanation for this finding is that younger patients are more concerned about cosmetic outcome and would be more interested in having breast reconstruction. Conversely, this finding may be related to the increasing number of comorbidities associated with increasing age, which could limit reconstruction in older age groups. The exact reasons for the lower rate of reconstruction among older women are unknown, but likely involve both patient preferences and/or biases of physicians.
Socioeconomic factors have also been shown to play a significant role in influencing reconstruction rates in that women with greater financial means more often have reconstruction. A 2001 US study found that women who earned more than US$40,000 were more likely to undergo breast reconstruction. In Western Australia and England, studies that used area code or educational level as proxies for socioeconomic status similarly found that women with lower incomes were less likely to have breast reconstruction. It has been shown that women with low incomes are less likely to have a physician-patient discussion regarding breast reconstruction and women of low income may be less aware of reconstructive options. Reconstruction also adds to recovery time with subsequent time away from work.
In addition, it is internationally well recognized that smoking correlates strongly with low socioeconomic status. It contributes to cardiovascular and respiratory related comorbidity that can strongly influence anaesthetic and surgical decision making. Smoking also compromises wound healing and increases post operative complication rates significantly. In many centres cigarette smoking is considered an absolute contraindication to advanced reconstructive techniques.
In Australia, reconstructive surgery is available in both the public and the private sectors, although it is more likely to be undertaken in the private sector. Whether this is by patient choice, education, socioeconomic status or due to the recommendation of the surgeon is unknown.
Higher population density (i.e. urban setting) is associated with an increased likelihood of having reconstruction, both in Australia and the USA. This finding may possibly reflect the availability of plastic surgeons as well as other factors including travel times.
A recently published Victorian study which explored factors associated with the likelihood of reconstruction after mastectomy found that breast reconstruction following mastectomy for invasive breast cancer is strongly influenced by demographic factors in women in Victoria. Women who had reconstruction were younger, more highly educated ie educated beyond school, more likely to live in the metropolitan area and to have private health insurance. The Breast,2012.
Surgeon Factors
Surgeon input is of vital importance to the patient considering mastectomy with immediate reconstruction. Traditionally, many patients have been advised by their health care providers to wait until mastectomy and chemotherapy or radiation therapy are complete before considering reconstruction. After undergoing such physically and emotionally exhausting treatments, however, patients are often spent, and have little interest in undergoing another surgical procedure. Proper counselling by surgeons, including the explanation that immediate reconstruction is associated with no difference in recurrence or survival outcomes compared with delayed reconstruction or no reconstruction at all is essential to allay the fear of recurrence or death that often guides patients’ decision-making.
A recent questionnaire-based study of factors influencing mastectomy patients’ choices regarding reconstruction found that patients regarded their surgeon’s advice as the most important factor. Moreover, women in the study who chose to undergo reconstruction were more likely than women who chose mastectomy alone to identify their surgeon’s advice as the most important influencing factor. Ann Surg Onc,2004.

Hawley et al, 2006 showed that a breast surgeon’s propensity to refer patients with breast cancer to a plastic surgeon before surgical cancer treatment explained a substantial amount of
between-surgeon variation in the use of reconstruction. A 2007 study found that almost half of surgeons (44%) referred <25% of women undergoing mastectomy for a plastic surgical opinion regarding reconstruction prior to the mastectomy. High-referral surgeons were more likely to be women and to have a high volume breast surgery practice. Cancer,2007.
A 2012 study demonstrated that the breast surgeon’s decision to refer a patient for reconstruction significantly affects whether the patient will undergo breast reconstruction. The results suggested that breast surgeons play a major role in determining whether or not a patient will ultimately undergo reconstruction. If the patient is not referred for consultation with a plastic surgeon, it is unlikely that the patient will independently seek out reconstruction, highlighting the importance of breast surgeons as “gatekeepers” to breast reconstruction. JAm Coll Surg,2012.
Take home message: You are much more likely to be referred to a plastic surgeon to discuss immediate reconstruction, and in turn, much more likely to undergo an immediate breast reconstruction, if you see a female specialist breast surgeon who performs a high volume of breast procedures annually!

Local Breast Reconstruction Rates
Jane O’Brien has an exceptionally high reconstruction rate. A personal practice audit of the last 3 years (2010-2012) revealed that over this period of time 65% of women diagnosed with breast cancer undergoing mastectomy underwent immediate reconstruction. This very high rate is explained by a number of factors, both physician, practice and patient related.
Jane O’Brien routinely discusses the option of breast reconstruction with all patients undergoing mastectomy, and our breast care nurses provide patients with written information /DVDs. Being a female breast surgeon who performs a high volume of cases annually, Jane fits the profile outlined above for high levels of onward referral to a plastic surgeon to discuss reconstructive options, which has also been shown to result in higher rates of immediate reconstruction. The Epworth Breast Service is a metropolitan, private practice, both features shown on Australian National Breast Cancer Audit data to be associated with higher levels of reconstruction.

The sociodemographic features of Jane O’Brien’s patient population overlap considerably with factors known to be associated with higher rates of reconstruction ie younger age, private health insurance, lower level of medical comorbidities.
Jane treats a large number of younger breast cancer patients. For example, although breast cancer occurs rarely in very young women, usually arbitrarily defined as those 35 years of age and under, with only about 2% of patients in this age group at diagnosis, Jane O’Brien treated a total of 21 patients aged 35 years and under over the five year period 2008-2013. A retrospective review of these women aged 35 years and under diagnosed with operable breast cancer and treated by Jane O’Brien over the five year period, revealed an immediate reconstruction rate of 100% with 11/21 (52%) patients undergoing mastectomy, ALL of whom underwent immediate reconstruction.
Jane’s patient group as a whole tends to be very health conscious, with a very low rate of smoking compared to the general population, and generally low levels of medical comorbidities which can serve as a relative contraindications to immediate reconstruction.

In summary, breast reconstruction involves complex decision making, however quality-of-life gains can be immensely rewarding. Whether a patient desires reconstruction at the time of mastectomy or years later, it is virtually always possible to find a reconstructive option that will work for her.