


Oncoplastic Breast Surgery
Breast surgeons have a new hat to wear if they choose, that of Oncoplastic Surgeon, using plastic surgical techniques to improve cosmetic outcomes in breast conservation surgery. Integrating oncoplastic techniques into breast conservation surgery can allow wider excision, expanding the limits of breast conservation in some cases, while preventing some of the cosmetic deformities.
Oncoplastic surgery of the breast is an innovative approach to the treatment of breast cancer. The word ‘oncoplastic’ is derived from the Greek words ‘onco’ (tumour) and ‘plastic’ (to mould). The concept encompasses the use of plastic surgical techniques in order to reshape the remaining breast or reconstruct the breast after appropriate wide excision of the breast cancer. The result is “seamless” specialist breast cancer surgery in which removal of the cancer is merged with reconstruction. This obviously requires very careful planning, and the delicate balancing of oncological needs with aesthetic aims.
The aim of any surgical technique in treating breast cancer is to remove the whole tumour with a clear margin of healthy tissue around it. In breast conserving surgery, a conflict exists between having a wide enough resection to obtain optimal oncological control and not removing so much breast tissue as to leave a deformed or asymmetric breast. Oncoplastic surgery has emerged as a new approach for extending breast conserving surgery possibilities, potentially reducing both mastectomy and reexcision rates, while avoiding breast deformities.
In a typical lumpectomy the surgeon makes an incision, excises the cancerous tissue and then closes the opening. This can often leave the breast with a disfiguring dent and there is a growing awareness that we haven’t always done as good a job as we should in offering aesthetic options to breast cancer patients in this situation. In fact, a recent study showed that around one third of patients are unhappy with the cosmetic outcome of their breast conserving surgery. Aesthetic Surg J 2008. To see some examples of what Miss O’Brien would regard as poor cosmetic outcomes following lumpectomy click here.
The oncoplastic breast surgeon must think, “How can I remove this cancer, achieving a satisfactory margin of normal tissue whilst at the same time making the patient look as good or even better than she looks now?” The ultimate oncoplastic achievement is to convert what would be, using standard surgical techniques, an oncologic and/or cosmetic failure, into both an oncologic and cosmetic success. Avoiding mastectomy, when it seems inevitable, in a patient who desires breast conservation, and ending up with an excellent cosmetic result, is one way to achieve that goal.

If you are faced with having to have breast cancer surgery, the aesthetic (cosmetic) outcome may well be the last thing on your mind. It is however accepted that any deformities are best treated at the time of original surgery for breast cancer excision. This is because it is more difficult to correct a deformity, especially after radiotherapy to the breast, than to prevent it, and also because the results of secondary corrective surgery are often not as good.
Oncoplastic breast surgery is a relatively new and rapidly growing field of surgery, and the number of surgeons trained in, and routinely using oncoplastic techniques in Australia is currently very low. The term ‘oncoplastic” only first appeared in the literature in 1996. This specialized field of surgery, initially confined to surgeons practicing in Europe, has more recently also gained popularity and attention in the United States.
Miss Jane O’Brien is currently one of a limited number of Australian breast surgeons trained and experienced in oncoplastic techniques. She underwent training and gained extensive surgical experience in these breast reconstructive techniques during her eight years of breast surgical practice in the United Kingdom (1996-2004) and has retained a very strong interest in this evolving field since returning to Australia. She has extensive experience in “oncoplastic” techniques and a significant proportion of her current surgical practice is now made up of oncoplastic breast surgical procedures. Although there is no professional certification for oncoplastic surgery, the American Society of Breast Surgeons and the American Society of Breast Disease both offer formal oncoplastic training courses for surgeons and Miss Jane O’Brien has completed both of these American oncoplastic courses (See Courses).

Traditionally, surgeons who treated breast cancer were taught how to remove the cancer, but nothing about the reconstructive aspects of surgery. Unless your breast surgeon has undergone additional training in this area it is unlikely that he/she will be in a position to offer you all the surgical options that are outlined below. As there is no professional certification for oncoplastic surgeons, patients should inquire specifically about practitioners’ training and experience in the area.
Oncoplastic surgery is more technically complex and does take more time to carry out than conventional breast surgery. It offers greater choice to women with breast cancer, extending the role of breast conserving surgery without cosmetic or oncological penalties and as such it will increasingly become patient driven and demanded. If surgeons are not in a position to offer oncoplastic techniques, their patients will drift away to surgeons who do. With patient related outcomes rightly at the heart of the agenda, the availability of oncoplastic surgery should be considered as a benchmark standard in the delivery of a modern breast service.
Oncoplastic breast-conservation surgery combines oncologic principles with plastic surgical techniques, but it is much more than a combination of two disciplines; it is a philosophy that requires vision, passion, knowledge of anatomy, and appreciation and understanding of aesthetics, symmetry, and breast function. The term oncoplastic surgery does not refer to any given surgical procedure but rather defines an approach and a surgical mindset to decision making and execution for all breast surgery. Oncoplastic breast surgeons have a commitment to aesthetics that takes into consideration the cosmetic repercussions of all breast operations, not just major resections.
This is true for even the smallest breast cancer lumpectomy procedure that may be regarded as potentially straightforward, and not requiring any specific cosmetic consideration. When carrying out any breast surgical procedure, it is important to give due consideration to the site and size of any incision, as it is may only be the scar that remains visible as a marker of surgery. Natural skin creases and lines of tension and can be used to guide optimal placement of incisions to result in neat, well-healed scars. The placement of scars outside the bra or in the cleavage area or décolletage should be avoided if possible. Incisions near the midline or overlying the sternum should similarly be avoided unless essential given their propensity to form hypertrophic or even keloid scars. Consideration should be given when planning the incision for breast conserving surgery as to how the incision can potentially be incorporated into a subsequent mastectomy (with immediate reconstruction if the patient desires) if operative pathology indicates that mastectomy is oncologically indicated.

As outlined above at least 30% of women are dissatisfied with the cosmetic results of their standard lumpectomy surgery. The size of the tumour in relation to the size of the breast is the single most important factor when predicting the potential cosmetic result. Those most likely to have a poor result are those with a large percentage volume of excision. For example, a women with a C cup breast with a 2cm tumour is likely to obtain a better cosmetic result from breast conserving surgery than if she had a very small AA cup breast and the same sized breast cancer, as a smaller proportion of the total volume of her breast needs to be removed to achieve satisfactory tumour clearance.
Another factor that may lead influence cosmetic outcome is the location of tumour within the breast. When the tumour is located in the centre, inferior (lower) or medial (inner) parts of the breast, up to 50% of patients may have a cosmetically unacceptable result with breast conserving surgery. This may manifest itself as a concave deformity, skin puckering or nipple displacement/deviation.
In general, excision volumes greater than 10% of total breast volume for medial lesions and more than 20% for lateral (outer) lesions are likely to result in an unsatisfactory aesthetic outcome. Centrally placed cancers that require excision of the nipple are also often left with obvious asymmetry and distortion.
Studies have shown that another reason for inferior cosmesis after wide local excision is insufficient breast tissue remodelling performed at the time of surgery. While the tumour excision cavity will fill with seroma fluid if the breast tissue is not reopposed, and will produce an initially acceptable cosmetic result in the short term, major deformities are seen in the longer term. In contrast to the old axiom “the seroma is your friend” the exact opposite is actually true. The results also become worse with post-operative radiotherapy which is routinely given after wide local excision of both pre invasive and invasive breast cancer.
As overall survival following breast cancer treatment improves, many women will be expected to live a long time with the cosmetic consequences of breast cancer surgery and improving cosmetic outcomes should be one of the main aims of breast cancer surgery.
Selection of patients for oncoplastic surgery
The question “Who is a good candidate for oncoplastic surgery?” is to a certain degree erroneous, because integration of surgical oncology with plastic and reconstructive surgery principles is applied to all patients by breast surgeons trained in oncoplastic surgery.
Most patients deemed eligible for breast conserving surgery will have a favourable tumour to breast size ratio and be suitable for conventional forms of wide local excision in which the tumour is excised with an approximately 1 cm margin of surrounding breast tissue. Though a re-excision may be required in a proportion of cases to achieve microscopically clear radial resection margins (at least 1 mm), an optimal cosmetic outcome should be attainable in the longer term after radiotherapy to the breast in most cases. Conversely, mastectomy is clearly indicated in some patients on the basis of tumour size and/or location, multifocality or patient choice.
Between these two extremes is a ‘grey area’ in which the limits of breast conserving surgery are being approached. For these patients, there is a risk that the tumour cannot be adequately excised without cosmetic detriment. It becomes progressively more difficult to achieve a good cosmetic outcome as the proportion of breast tissue removed increases. Oncoplastic procedures permit wider resection of tissue, increasing the chance of obtaining tumour-free margins, but not at the expense of sacrificing the cosmetic outcome.
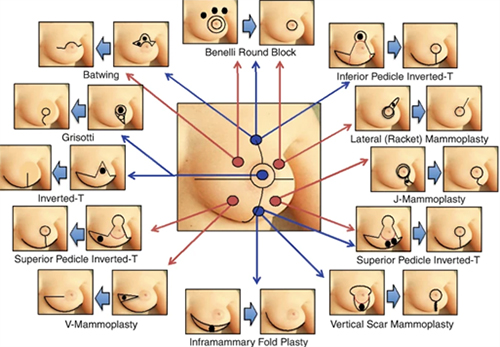
The choice of the reconstructive method
To determine which reconstructive option is best for the patient, the size and location of the expected tumour resection and the ratio of breast volume to resection volume must be appreciated.
|
LOCATION
|
PROCEDURES
|
|
Upper pole |
Inferior pedicle inverted-T mammoplasty Benelli round block Batwing mastopexy |
|
Upper outer quadrant |
Lateral (Racquet) mammoplasty Radial oblique incision Benelli round block |
|
Lower outer quadrant |
Superior pedicle inverted-T mammoplasty J-mammoplasty |
|
Lower pole |
Superior pedicle inverted-T mammoplasty Vertical scar mammoplasty Inframammary Fold Plasty |
|
Lower inner quadrant |
Superior pedicle inverted-T mammoplasty V-mammoplasty |
|
Upper inner quadrant |
Benelli round block Batwing mastopexy
|
|
Central quadrant |
Periareolar excision closed in a straight horizontal line or in a purse-string manner Inverted-T/vertical-scar mammoplasty with/without NAC resection Grisotti technique |
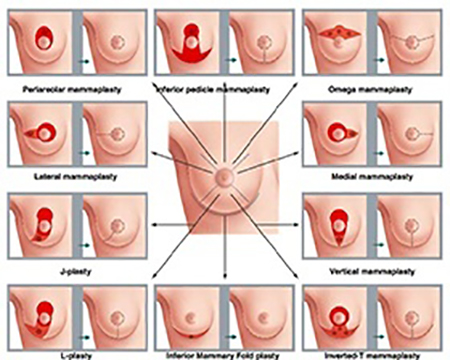
Classification of Oncoplastic Breast Surgery techniques according to Tumour Location
Techniques of oncoplastic surgery
Oncoplastic surgery in the context of partial breast reconstruction encompasses both volume replacement and volume displacement techniques. The former imports additional tissue from outside the breast in the form of a tissue flap to compensate for loss of volume from surgical excision. In contrast, the latter (volume displacement) rearranges the remaining breast tissue, and the volume loss is thereby absorbed over a wider area with concomitant re-shaping of the breast. Volume displacement represents the simplest option for partial breast reconstruction and is usually preferred over techniques for volume replacement which involve more extensive surgery with harvesting of a myocutaneous or subcutaneous flap. These flaps cannot then subsequently be used for whole-breast reconstruction should the patient develop local recurrence and require mastectomy.
Volume displacement techniques
Several options are available for volume displacement which constitutes a spectrum of techniques of varying complexity The common aim of volume displacement is to utilise the remaining breast tissue to fill the defect resulting from excision of the tumour. As previously discussed, resections which lead to loss of >10-20% of breast volume are likely to incur significant cosmetic detriment and to demand some form of ‘infill’ to create an acceptable cosmetic outcome in the longer term. Displacement techniques re-shape the breast through advancement, rotation or transposition of existing parenchyma and skin with a resultant decrease in overall breast volume.

There are numerous oncoplastic volume displacement options. They include:
1. Upper pole of breast
(a) Crescent Mastopexy
(b) Batwing Resection
(c) Hemibatwing Resection
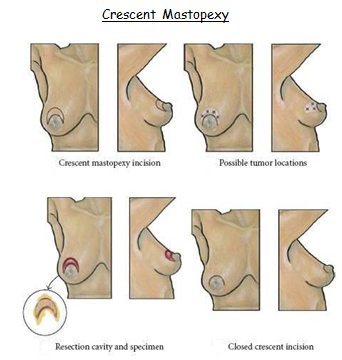
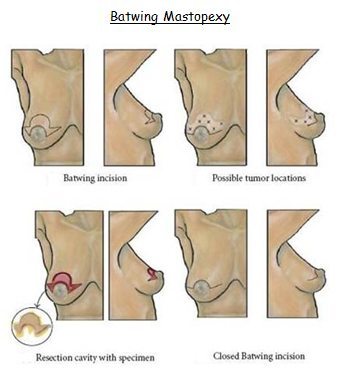
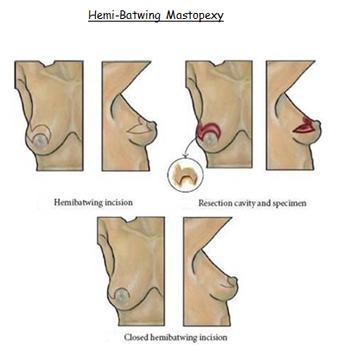
For lesions in the upper hemisphere (10 o’clock to 2 o’clock going clockwise), crescent, batwing or hemi-batwing excisions can be used. They work well for patients with larger, more ptotic breasts who will benefit from lifting the nipple areolar complex. These incisions allow the cancer to be generously removed while allowing recontouring the breast in a desirable fashion. All lift the nipple areola complex.
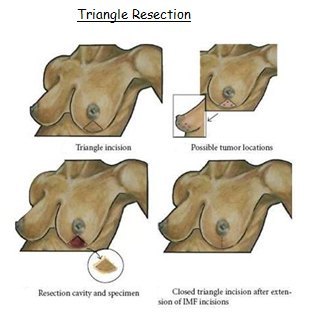
2. Lower pole of breast
(a) Triangle Incision
(b) Reduction Mastopexy
(c) Inframammary (does not remove skin)
For lesions in the lower hemisphere of the breast a standard breast reduction incision works well. This allows access to lesions from 3 o’clock to 9 o’clock, going clockwise. Large amounts of breast tissue can be removed with excellent cosmetic results and generally widely clear margins.
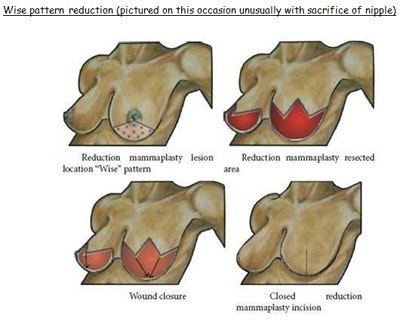
3. Any segment of the breast
(a) Radial–ellipse segmentectomy
(b) Circumareolar approach for segmental resection (does not remove skin)
(c) Donut or round block mastopexy
(d) Wise pattern reduction
All images sourced: Holmes et al, 2011
The Other Breast
When symmetry is desired, the contralateral breast may need to be adjusted. This can be done during the same operative procedure as the initial cancer or preferably as a delayed procedure. The advantage of doing both sides simultaneously is a single operative procedure. The disadvantage is that the final pathology and, in particular, the margin status is unknown before altering the appearance of the opposite breast. In addition, the effect of radiotherapy on the treated breast is variable and unpredictable. In some cases radiotherapy leads to significant shrinkage, in others persistent oedema (swelling) and for this reason it may be preferable to delay a symmetrisation procedure to the other breast until the treated breast has settled down post radiotherapy which usually takes at least six- twelve months following completion of treatment.
REFERENCES:
![]() Oncoplastic breast-conserving surgery
Oncoplastic breast-conserving surgery
VIDEOS
Oncoplastic and Reconstructive Breast Surgery explained
Oncoplastic Breast Cancer Surgery
Oncoplastic Techniques
You will need the Adobe Reader to view and print these documents.
![]()
Error: Contact form not found.